


Will artificial intelligence replace surgeons? A thoracic surgeon’s perspective
 0
0 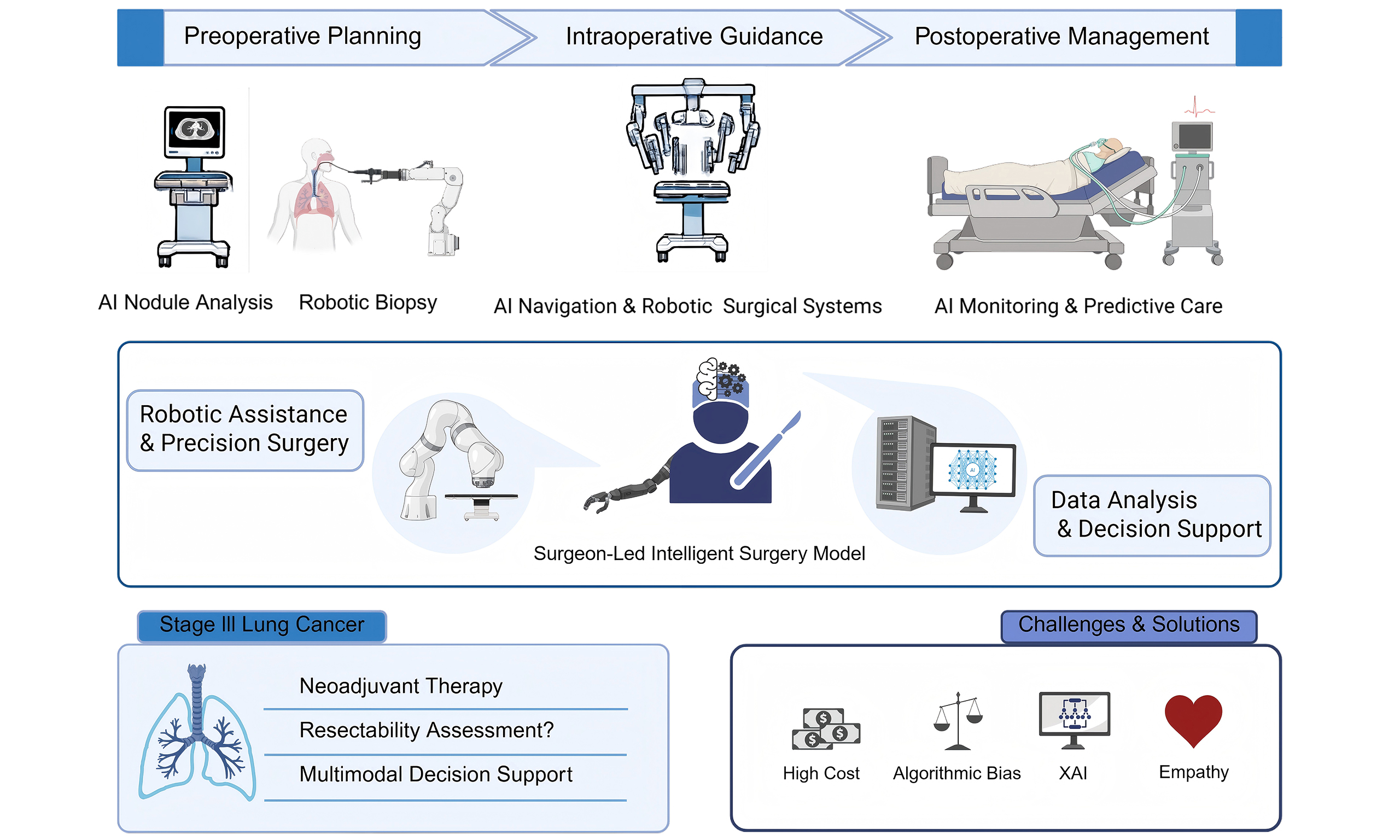
THE WIDESPREAD INTEGRATION OF AI IN THORACIC SURGERY
Artificial intelligence (AI) has progressed from a theoretical concept to a fundamental component of the entire perioperative patient care continuum[1]. This advancement has been primarily driven by two factors: improvements in algorithmic capabilities and the clinical integration of surgical robotic systems.
Machine learning (ML)-based algorithms serve as the foundation for achieving high diagnostic accuracy and enabling tailored treatment strategies. In thoracic surgery, many new models are being developed to support lung cancer diagnosis, predict lymph node metastasis and assess the risk of postoperative complications[2]. For example, by leveraging clinical data, a machine-learning model can predict the risk of prolonged air leak after a lung resection with an Area Under the Curve (AUC) of 0.84. Such accurate prediction could substantially aid surgeons in proactively managing PAL in patients undergoing video-assisted thoracoscopic surgery (VATS)[3]. As validation study results continue to accumulate, leading medical centers are progressively incorporating these models into their clinical platforms.
Operationally, as the essential hardware platform for implementing AI, surgical robots are experiencing steadily increasing rates of installation and utilization. In the United States, the proportion of lobectomies performed via Robot-Assisted Thoracoscopic Surgery (RATS) increased from 19.2% to 34% between 2015 and 2018[4]. This upward trend continues globally, with robotic surgery gradually transitioning from an alternative approach to a mainstream modality in thoracic surgery[5].
FROM MASTER-SLAVE TO PARTNERSHIP: THE EVOLVING TRIPARTITE RELATIONSHIP
The Da Vinci Surgical System, based on a “master-slave” design[6], enhances surgical stability and dexterity. Nevertheless, the quality and efficiency of surgery remain dependent on the surgeon’s expertise and endurance. The incorporation of increasingly advanced AI as a core processor is expected to endow these systems with greater autonomy, enabling a phased transition from teleoperation (L0) and task assistance (L1-L3) to conditional autonomy[7]. The integration of advanced algorithms with hardware platforms has laid a solid foundation for the development of an intelligent surgical model characterized by tripartite collaboration. This model, designed to enhance the surgeon’s strategic decision-making while leveraging AI and robotic systems as capability extensions, constitutes a dataflow-driven closed-loop system that is fundamentally transforming the paradigm of clinical practice in thoracic surgery.
The following sections discuss the specific applications of this model in preoperative planning, intraoperative guidance, and postoperative management, highlighting both current applications and future prospects of this tripartite collaboration [Figure 1].
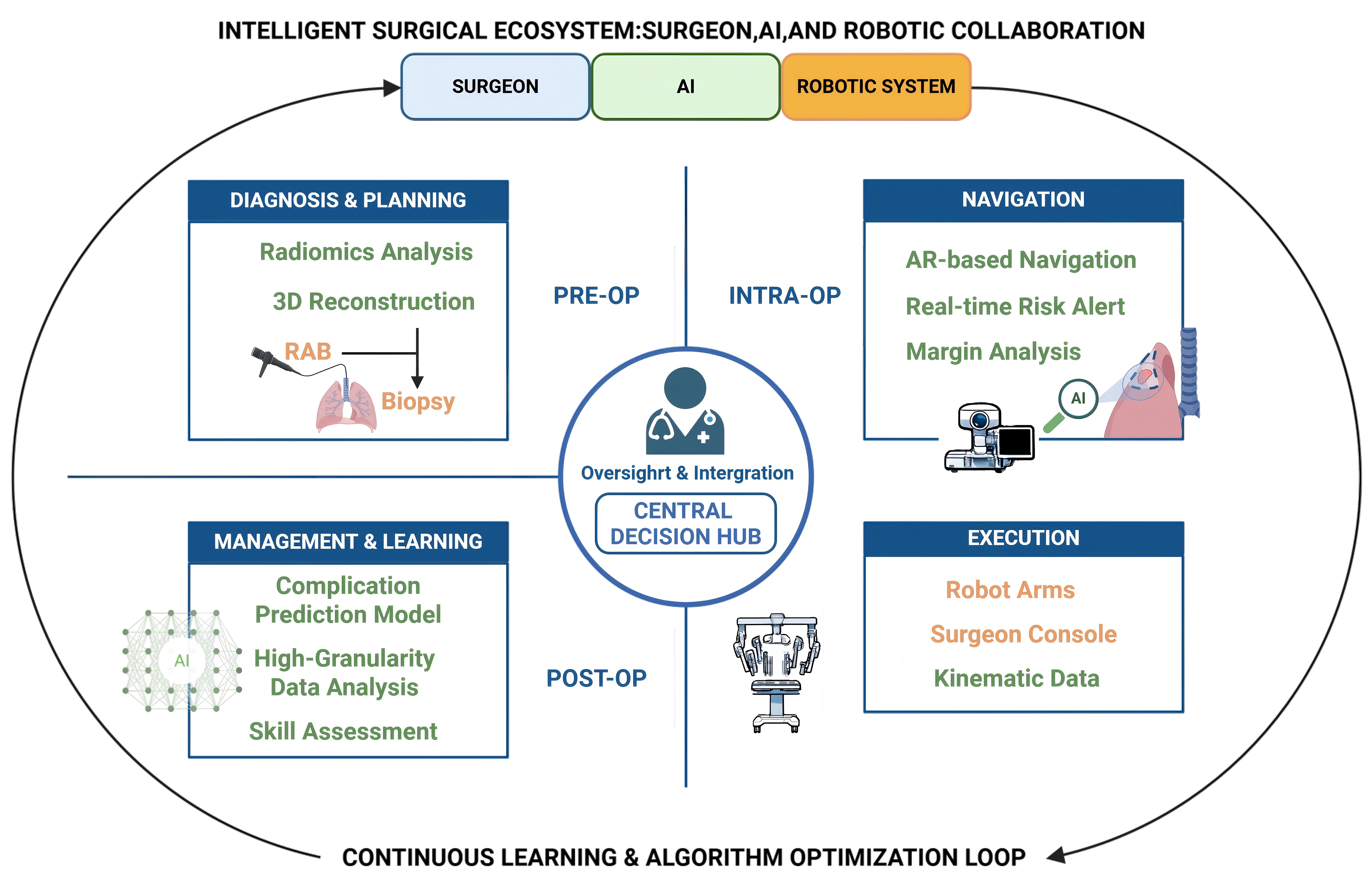
Figure 1. Tripartite collaboration among AI, robotic systems, and surgeons is reshaping the perioperative workflow of thoracic surgery, creating a dynamic, efficient, and mutually reinforcing closed-loop system (Created with BioRender.com, link: https://BioRender.com/qroije1). AI: Artificial intelligence; RAB: robot-assisted bronchoscopy; AR: augmented reality.
THE INTELLIGENT SURGERY MODEL: PERIOPERATIVE APPLICATIONS
Preoperative diagnosis and surgical planning
Radiomic models facilitate high precision and non-invasive differentiation between malignant and benign pulmonary nodules by identifying subtle imaging features[8]. A model developed by Ardila et al. achieved a state-of-the-art performance (94.4% area under the curve) in 6,716 cases from the National Lung Screening Trial, thereby helping improve the accuracy and efficiency of lung cancer screening[9]. For peripheral nodules classified as “high risk”, robot-assisted bronchoscopy (RAB) offers distinct advantages. This system combines three-dimensional image navigation with a highly flexible and stable robotic catheter, enabling precise guidance of biopsy instruments directly to the target lesion. A study by Paez et al. demonstrated that RAB achieved diagnostic accuracy that was at least noninferior, and possibly superior, to that of traditional techniques such as electromagnetic navigation bronchoscopy, with a noninferiority P value of 0.007, while maintaining an excellent safety profile[10].
Once a definitive diagnosis is provided by a pathologist, the surgeon develops a precise operative plan. This individualized surgical strategy is based on a 3D reconstruction generated from the patient’s lung Computed Tomography (CT) scan[11]. With AI assistance, surgeons can more effectively determine the optimal surgical approach, incision site, and extent of resection (lobectomy vs. sublobar resection), as well as identify anatomical variations.
Intraoperative guidance and precision resection
Robotic systems can provide a stable working environment when performing dissections in anatomically challenging areas. Research by Nelson et al. demonstrated that robotic-assisted lobectomy (RAL) was associated with longer operative times, reduced blood loss, improved lymph node harvest (all P < 0.02), and a shortened hospital stay[12]. AI further enhances robotic surgical systems by improving perception and enabling intelligent navigation. Augmented reality (AR) can delineate tumor margins and vascular structures by overlaying preoperative imaging data onto the surgical field[13]. Moreover, algorithms that track tissue displacement caused by physiological movements, such as respiration, enable precise intraoperative navigation. Looking ahead, AI may integrate intraoperative three-dimensional reconstruction with instrument tracking technology to enable real-time monitoring of surgical video feeds and vital signs, thereby predicting potential risks.
Postoperative management and learning
Models trained on surgical, clinical, and pathological records can predict the risk of postoperative complications[14]. This enables surgeons to tailor their strategies to the monitoring and early intervention of patients identified as high-risk, thereby promoting precise and personalized postoperative care.
A data-driven positive feedback loop may emerge in this process. As high-resolution data generated by surgical robots is collected[15] and continuously refines the algorithm, AI will be capable of defining objective assessment criteria for surgical abilities. This capability, in turn, may provide a novel approach to improving surgical performance and training[15].
CONTROVERSIES AND GAPS: THE DEEPENING APPLICATION OF INTELLIGENT SURGERY
Stage III lung cancer, characterized by its high heterogeneity and substantial therapeutic challenges, remains the most formidable issue in contemporary lung cancer management and represents a particularly promising application scenario for the intelligent surgical model. Beyond optimizing the surgical procedure itself, this model has the potential to support the development of personalized therapeutic strategies for patients with locally advanced disease. With a properly sequenced regimen of neoadjuvant therapy and surgery, patients may achieve long-term survival.
For patients who have undergone neoadjuvant therapy, VATS presents increased technical difficulty. In contrast, RATS systems have demonstrated superior clinical outcomes, including reduced operative time, a lower conversion rate to open thoracotomy, and enhanced efficiency in lymph node dissection[16]. Moreover, AI shows considerable potential in assisting surgeons with complex or controversial surgical decision-making. Previous studies have demonstrated that a CT-based deep learning approach (the NeoPred model) can predict response to immunotherapy in patients with non-small cell lung cancer (NSCLC)[17]. However, a critical gap remains: no study has yet integrated clinical characteristics, CT imaging, and pathological features to develop a comprehensive multimodal model. By combining AI predictions with clinical expertise, clinicians may more accurately identify patients with complete treatment response. For these individuals, surgeons may adopt personalized strategies, such as deviating from the standard of care based on pre-therapy tumor staging by avoiding radical pneumonectomy. Furthermore, the definition of “borderline resectable” remains subjective, often reliant on the surgeon’s personal judgment[18]. Through analysis of extensive clinical datasets, AI holds the potential to uncover complex patterns associated with R0 resection and long-term survival, thereby facilitating the development of personalized resectability scoring systems. Going a step further, AI could support feasibility assessments for conversion surgery in patients initially deemed unresectable following induction therapy.
FROM OBSTACLES TO SOLUTIONS: EXPLORING A NEW SURGICAL ERA
Although the intelligent surgical model holds substantial clinical promise, key barriers remain at both the research and implementation stages. In particular, most studies of machine-learning predictive models are single-center and retrospective, and therefore provide only limited evidence. The lack of high-level, multicenter, prospective clinical validation hinders their adoption in clinical practice and prevents their incorporation into clinical guideline development. Furthermore, predicted outcomes often focus on perioperative short-term metrics, lacking assessment data on patients’ long-term survival and quality of life.
The critical obstacles in the implementation phase are primarily manifested in technological, ethical, and humanistic aspects.
For instance, inequitable access to robotic and AI technologies is driven largely by their high cost. A fundamental question of social justice is: who stands to gain from these technological advances? Their concentration in economically developed regions may exacerbate global health disparities and result in tangible harm[19]. Mitigating this requires cost reduction through international collaboration. This gives rise to a second issue: data bias. Information from developed regions may lack generalizability, thereby compromising algorithmic fairness[20]. Future initiatives should focus on establishing high-quality global surgical databases. Furthermore, reliance on “black-box” algorithms creates major concerns regarding transparency[21]. Developing explainable AI (XAI) and establishing a robust medical AI validation and regulatory framework may help increase physicians’ confidence in these new technologies.
As robotic autonomy advances, the ethical issue of accountability becomes more prominent. Similar to the issue of determining liability in an accident involving an autonomous vehicle[22], it is imperative to develop a robust legal and ethical framework to delineate rights and obligations in human-robot surgical collaboration and to ensure informed patient consent. The development of this framework should be guided by comprehensive societal dialogue[23].
As AI cannot address emotional problems, empathetic surgeons must retain the central role within the intelligent surgical model. Complete delegation of patient care to AI could diminish therapeutic adherence and negatively impact treatment outcomes. Addressing this challenge necessitates a redefinition of the surgeon’s role and a restructuring of medical education. Cancer treatment involves divergent patient priorities, ranging from accepting higher risks for potential survival gains to prioritizing quality of life. Fully autonomous, AI-driven surgery is fundamentally limited in addressing this spectrum of values. Accordingly, the empathy and emotional support provided by human physicians therefore remain an indispensable component of patient-centered care.
SUMMARY
For clarity, the AI-related topics discussed in this perspective are summarized in Table 1. In the foreseeable future, AI is more likely to augment rather than replace surgeons. A surgeon-led intelligent surgical model is emerging, in which AI and robotic systems empower and extend the capabilities of surgeons. High-quality real-world data will, in turn, support the development of more advanced algorithms and increasingly autonomous robotic systems. By addressing the challenges outlined above, this approach may foster a more natural, transparent, and trustworthy model of collaboration.
Categorization of AI-related content
| Category | Main content in this review | Representative examples in thoracic surgery | Current status |
| Current achievements of AI | AI has already been applied across the perioperative workflow and has shown measurable benefits in diagnosis, planning, and risk prediction | ML models for lung cancer diagnosis, lymph node metastasis prediction, and postoperative complication assessment; prediction of prolonged air leak; AI-assisted CT-based 3D reconstruction for surgical planning; robotic-assisted thoracic surgery and robotic-assisted bronchoscopy in clinical practice | Supported by existing retrospective and early clinical studies; some technologies have already entered real-world clinical use |
| Ongoing verification processes of AI | Many existing AI models remain under validation before routine adoption and guideline integration | Most prediction models are based on single-center retrospective studies; lack of multicenter prospective validation; limited evidence regarding long-term survival and quality-of-life outcomes; concerns regarding data bias, fairness, explainability, and regulatory oversight | Promising but not yet fully validated; requires higher-level clinical evidence and more robust governance frameworks |
| Future envisioned scenarios of AI | AI and robotic systems may evolve from assistive tools into more intelligent collaborative partners of surgeons | Increasing robotic autonomy; real-time integration of intraoperative 3D reconstruction, instrument tracking, and vital-sign monitoring for risk prediction; personalized resectability scoring; feasibility assessment for conversion surgery after induction therapy; a surgeon-led intelligent surgical model enabling precision and individualized care | Conceptual and forward-looking; not yet mature for widespread clinical implementation |
DECLARATIONS
Acknowledgments
We thank all members of our laboratory and team for their support throughout this research. The graphical abstract of this article was created with BioRender.com (https://BioRender.com/xrgnjcm).
Authors’ contributions
Made substantial contributions to the writing of the article: Wang Y, Song C, Mao W
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool DeepSeek (online version) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was partially supported by the Top Talent Support Program for Young and Middle-aged People of the Wuxi Municipal Health Commission (HB2020003) and the Mega-project of the Wuxi Commission of Health (Z202216).
Conflicts of interest
Mao W is a Junior Editorial Board Member of Mini-invasive Surgery and was not involved in any aspect of the editorial process for this manuscript, including reviewer selection, manuscript handling, or decision-making. The other authors declare that they have no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Leivaditis V, Maniatopoulos AA, Lausberg H, et al. Artificial intelligence in thoracic surgery: a review bridging innovation and clinical practice for the next generation of surgical care. J Clin Med. 2025;14:2729.
2. Li Y, Wu X, Yang P, Jiang G, Luo Y. Machine learning for lung cancer diagnosis, treatment, and prognosis. Genomics Proteomics Bioinformatics. 2022;20:850-66.
3. Tou S, Matsumoto K, Hashinokuchi A, et al. Data‐driven prediction of prolonged air leak after video‐assisted thoracoscopic surgery for lung cancer: development and validation of machine‐learning‐based models using real‐world data through the ePath system. Learn Health Syst. 2024;9:e10469.
4. Alwatari Y, Khoraki J, Wolfe LG, et al. Trends of utilization and perioperative outcomes of robotic and video-assisted thoracoscopic surgery in patients with lung cancer undergoing minimally invasive resection in the United States. JTCVS Open. 2022;12:385-98.
5. Shanahan B, Galloway R, Stamenkovic S, et al. Thoracoscopic surgery in lung cancer: the rise of the robot. J Thorac Dis. 2023;15:5263-7.
6. Vasey B, Lippert KA, Khan DZ, et al. Intraoperative applications of artificial intelligence in robotic surgery: a scoping review of current development stages and levels of autonomy. Ann Surg. 2023;278:896-903.
7. Schmidgall S, Opfermann JD, Kim JW, Krieger A. Will your next surgeon be a robot? Autonomy and AI in robotic surgery. Sci Robot. 2025;10:eadt0187.
8. Pei Q, Luo Y, Chen Y, Li J, Xie D, Ye T. Artificial intelligence in clinical applications for lung cancer: diagnosis, treatment and prognosis. Clin Chem Lab Med. 2022;60:1974-83.
9. Ardila D, Kiraly AP, Bharadwaj S, et al. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat Med. 2019;25:954-61.
10. Paez R, Lentz RJ, Duke JD, et al. Robotic versus electromagnetic bronchoscopy for peripheral pulmonary lesions: a randomized trial (RELIANT). Am J Respir Crit Care Med. 2025;211:1644-51.
11. Chen X, Dai C, Peng M, et al. Artificial intelligence driven 3D reconstruction for enhanced lung surgery planning. Nat Commun. 2025;16:4086.
12. Nelson DB, Mehran RJ, Mitchell KG, et al. Robotic-assisted lobectomy for non-small cell lung cancer: a comprehensive institutional experience. Ann Thorac Surg. 2019;108:370-6.
13. Li D, Shan Y, Shi H, et al. A novel image-guided robotic system with motion compensation for intraoperative radiation-free localization of pulmonary nodules. Med Image Anal. 2025;105:103691.
14. Peng S, Jia K, Peng M, et al. Predicting NSCLC surgical outcomes using deep learning on histopathological images: development and multi-omics validation of Sr-PPS model. Int J Surg. 2025;111:4279-94.
15. Knudsen JE, Ghaffar U, Ma R, Hung AJ. Clinical applications of artificial intelligence in robotic surgery. J Robotic Surg. 2024;18:102.
16. Li HJ, Ding JY, Nie Q, et al. Advantages of robotic-assisted thoracic surgery after neoadjuvant therapy in NSCLC: a propensity score–matched analysis. Eur J Surg Oncol. 2025;51:110022.
17. Zheng J, Yan Z, Wang R, et al. NeoPred: dual-phase CT AI forecasts pathologic response to neoadjuvant chemo-immunotherapy in NSCLC. J Immunother Cancer. 2025;13:e011773.
18. Aigner C, Baldes N, Begic M, Doerr F, Hoda MA, Bölükbas S. Current perspective on resectability in stage III locally advanced NSCLC - the thoracic surgeons’ view. Eur J Cancer. 2025;221:115426.
19. Weber M, Park KB, Afshar S. Equalizing access: how robotics and AI can transform surgical care worldwide. Sci Robot. 2025;10:eadt6471.
20. Chen RJ, Wang JJ, Williamson DFK, et al. Algorithmic fairness in artificial intelligence for medicine and healthcare. Nat Biomed Eng. 2023;7:719-42.
21. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25:44-56.
22. Rivero-Moreno Y, Rodriguez M, Losada-Muñoz P, et al. Autonomous robotic surgery: has the future arrived? Cureus. 2024;16:e52243.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].